")
The 2026 ACC/AHA Cholesterol Guidelines: What Every Patient Should Know
March 23, 2026

The 2026 ACC/AHA cholesterol guidelines changed how heart risk is assessed. Learn the key updates and how NiuOla Health in Olympia, WA can help you take action.
The Cholesterol Rules Just Changed, Here’s What It Means for You
On March 13, 2026, the American College of Cardiology and the American Heart Association released the most significant update to cholesterol guidelines since 2018. These changes affect how your doctor evaluates your heart disease risk, when treatment is recommended, and what goals you’re working toward together.
At NiuOla Health, Dr. Tui Lauilefue is already applying these updates in practice. Here’s what you need to know.
A Smarter Way to Calculate Your Risk
The 2026 guidelines replace older risk calculators with the PREVENT equations. It’s a more accurate tool that factors in kidney health, metabolic conditions, and long-term risk. Previous calculators overestimated cardiovascular risk by 40–50%.
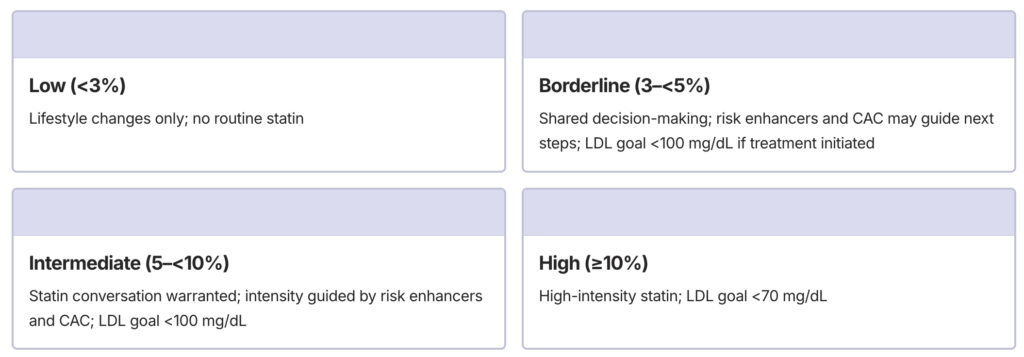
The PREVENT equations estimate absolute 10–year risk for total CVD (PREVENT-CVD), ASCVD (PREVENT-ASCVD) and HF (PREVENT-HF) for adults aged 30–79 years and 30-year risk for total CVD among adults aged 30–59 years. For younger adults whose 10-year number looks low, the 30-year estimate often tells a more complete story.
Risk categories and treatment defaults:
Some Patients Skip the Calculator Entirely
PREVENT is for primary prevention only. People without existing heart disease. If you fall into any of the categories below, treatment is automatic:
- Existing Cardiovascular Disease
- High-intensity statin; LDL goal as low as <55 mg/dL
- LDL ≥190 mg/dL
- High-intensity statin plus additional agents if needed
- Diabetes (ages 40–75)
- At minimum a moderate-intensity statin
- Chronic Kidney Disease (Stage 3-4)
- Moderate-intensity statin therapy (or moderate-intensity statin combined with ezetimibe) for adults 40–75 years with CKD stage 3 or higher and LDL-C 70–189 mg/dL
- HIV (ages 40–75)
- Statin recommended regardless of risk score; pitavastatin preferred due to fewer drug interactions
For these patients, the question isn’t whether to treat—it’s how aggressively.
2026 Guidelines
Coronary Artery Calcium Scoring: Clarity When You Need It Most
For borderline or intermediate-risk patients unsure about starting a statin, coronary artery calcium (CAC) scoring is one of the most valuable tools the 2026 guidelines highlight.
A CAC scan is a fast, non invasive CT scan that detects plaque buildup inside your coronary arteries, often years before any symptoms appear. It answers a question no blood test can: what is actually happening inside my arteries right now?
The guidelines recommend CAC for men ≥40 and women ≥45 with borderline or intermediate risk when the decision is uncertain:
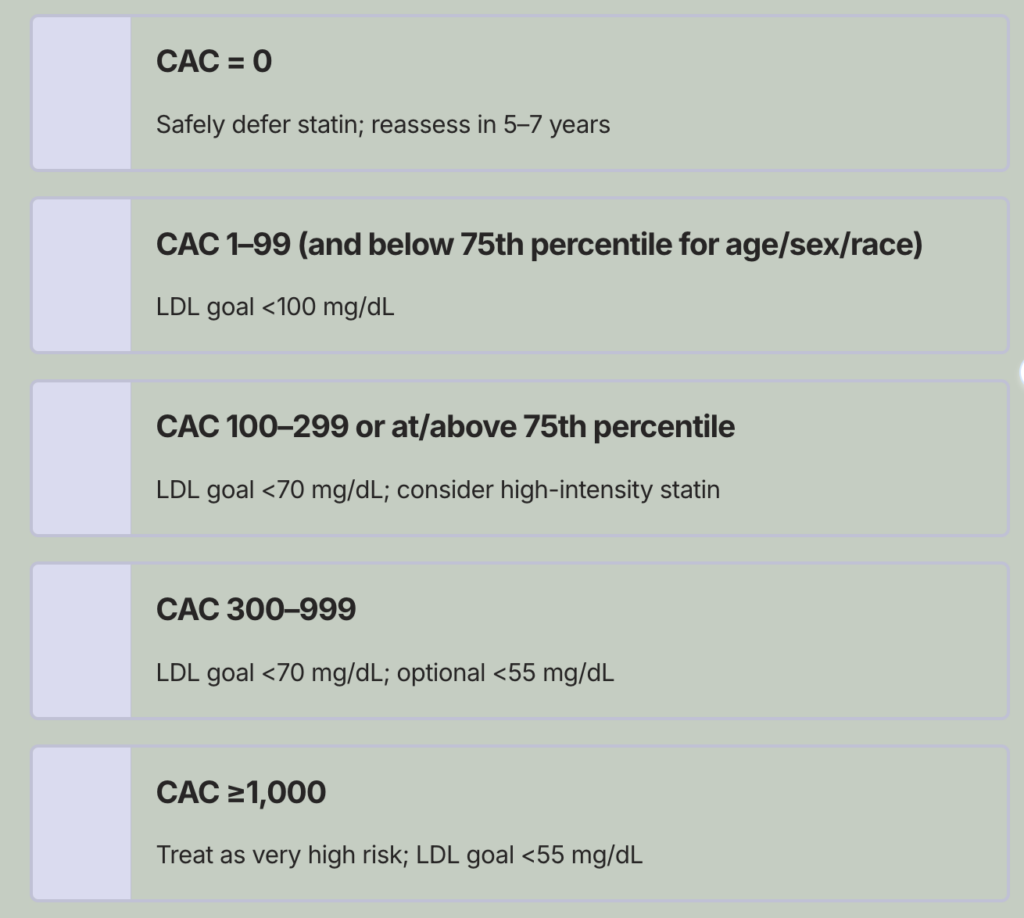
A score of zero brings real reassurance. A higher score removes the guesswork and creates a clear, personalized path forward.
Important Biomarkers to Ask About
Lp(a)
Now a Class I recommendation: every adult should have this measured once in their lifetime. It’s genetically determined, won’t show up on a standard cholesterol panel, and levels ≥125 nmol/L significantly raise cardiovascular risk.
ApoB
Useful when standard LDL may underestimate risk especially with metabolic syndrome, high triglycerides, or low HDL.
hsCRP
A marker of inflammation that can help clarify borderline or intermediate treatment decisions.
If your Lp(a) has never been checked, ask at your next visit.
Risk Enhancers That Can Change Your Treatment Path
For borderline or intermediate patients, certain factors can appropriately shift the recommendation toward treatment:
Lab & Metabolic Factors
- LDL-C ≥160 mg/dL or non-HDL-C ≥190 mg/dL
- Triglycerides ≥175 mg/dL
- ApoB ≥130 mg/dL
- Lp(a) ≥125 nmol/L (50 mg/dL) raises risk; ≥250 nmol/L (100 mg/dL) roughly doubles it
- hsCRP ≥2.0 mg/L
- Metabolic syndrome
- Chronic kidney disease (non-dialysis, stage 1–2)
Clinical & Personal History
- Inflammatory conditions: rheumatoid arthritis, psoriasis, lupus
- Premature menopause (before age 40) or history of preeclampsia or eclampsia
- South Asian or Filipino ancestry (including individuals with heritage from India, Pakistan, Bangladesh, Sri Lanka, Nepal, or Bhutan) — this group carries higher ASCVD risk at lower traditional risk factor levels than PREVENT equations may predict
- Ankle-brachial index <0.9
- Family history of premature cardiovascular disease (heart attack or stroke in a first-degree male relative before age 55, or female relative before age 65)
These factors don’t automatically trigger treatment, but they meaningfully inform the conversation.
Metabolic Health and Cholesterol Are One Conversation
The 2026 guidelines formally recognize cardiovascular-kidney-metabolic (CKM) syndrome, the cluster of abdominal obesity, insulin resistance, high triglycerides, low HDL, and elevated blood pressure that together dramatically raise cardiovascular risk.
- Heart-Healthy Nutrition
- Regular Movement
- Quality Sleep
- Tobacco Avoidance
- Stress Reduction
At NiuOla Health, your cholesterol isn’t reviewed in isolation. It’s evaluated alongside your metabolic health, weight, blood sugar, and lifestyle as one complete picture.
And regardless of medication, lifestyle remains the foundation for every patient:
Ready to Take the Next Step?
The 2026 guidelines are more personalized and more precise than ever but they only make a difference when applied to your life and your numbers.
As a direct primary care practice, NiuOla Health offers the time and relationship-centered care to do exactly that. Schedule a visit with Dr. Tui Lauilefue in Olympia, Washington to review your lipid panel, explore whether a CAC scan is right for you, and build a heart health plan grounded in the latest evidence.
